The U.S. Centers for Disease Control and Prevention has expanded its 30-day ban on entry to the United States to green card holders over the widening Ebola outbreak in central Africa.
The May 22 update, states that any foreign nationals or green card holders who have been in countries experiencing a known or suspected outbreak of Bundibugyo ebolavirus disease—the Democratic Republic of the Congo (DRC), Uganda, or South Sudan—at any point in the last 21 days, regardless of their country of origin, are suspended from entering the United States until June 17. At that time, the CDC will issue more detailed policy in response to the outbreak.
The CDC said the 30-day period will give acting director Dr. Jay Bhattacharya time to “make an informed determination” about necessary travel restrictions going forward.
U.S. citizens and U.S. nationals may still return from the countries of concern, but will face “enhanced public health entry screening.” However, the CDC warned that the screening is not able to identify “travelers who are infected but not yet showing symptoms,” as symptoms of Ebola can take up to 21 days to develop after initial exposure.
“Screening is one part of a broader, layered public health approach that also includes exit screening overseas, airline illness reporting, and public health monitoring after arrival,” the CDC said.
Arrivals from these countries will have their flights re-routed to arrive at select airports. “Some travelers may have an additional public health assessment if they have been in certain situations,” the agency added.
Those allowed to go home will be sent automated text messages with reminders to monitor their health and actions to take if symptoms develop. State and local health departments will be provided with traveler lists and contact information for additional follow-up and support.
The temporary measure is in place under Title 42 travel restrictions—the same authority used during the COVID-19 pandemic.
Ebola is a disease caused by orthoebolaviruses. It can cause common symptoms such as fever, aches, pains, and fatigue, and in severe cases, vomiting, and unexplained bleeding.
There have been two previous outbreaks of the rarer Bundibugyo ebolavirus, one in 2007 in Uganda with a mortality rate of 25 percent, and one in 2012 in the DRC with a 50 percent mortality rate. Bundibugyo has generally been associated with lower fatality rates than other strains of Ebola—though still very dangerous.
Zaire ebolavirus, which is the strain typically associated with Ebola outbreaks, is considered to have a mortality rate of 50–90 percent. It is the only strain for which vaccines and monoclonal antibody therapies have been developed, according to the Food and Drug Administration.
Earlier this week, a World Health Organization advisory group recommended testing the efficacy and safety of two monoclonal antibodies, one from Regeneron and one from Mapp Biopharmaceutical, in clinical trials against the virus, as well as looking at an antiviral called obeldesivir for post-exposure prophylaxis.
So far for this outbreak in the DRC and Uganda, there have been 88 confirmed cases, 750 suspected cases, 10 confirmed deaths, and 176 suspected deaths. The numbers are expected to rise as surveillance expands.
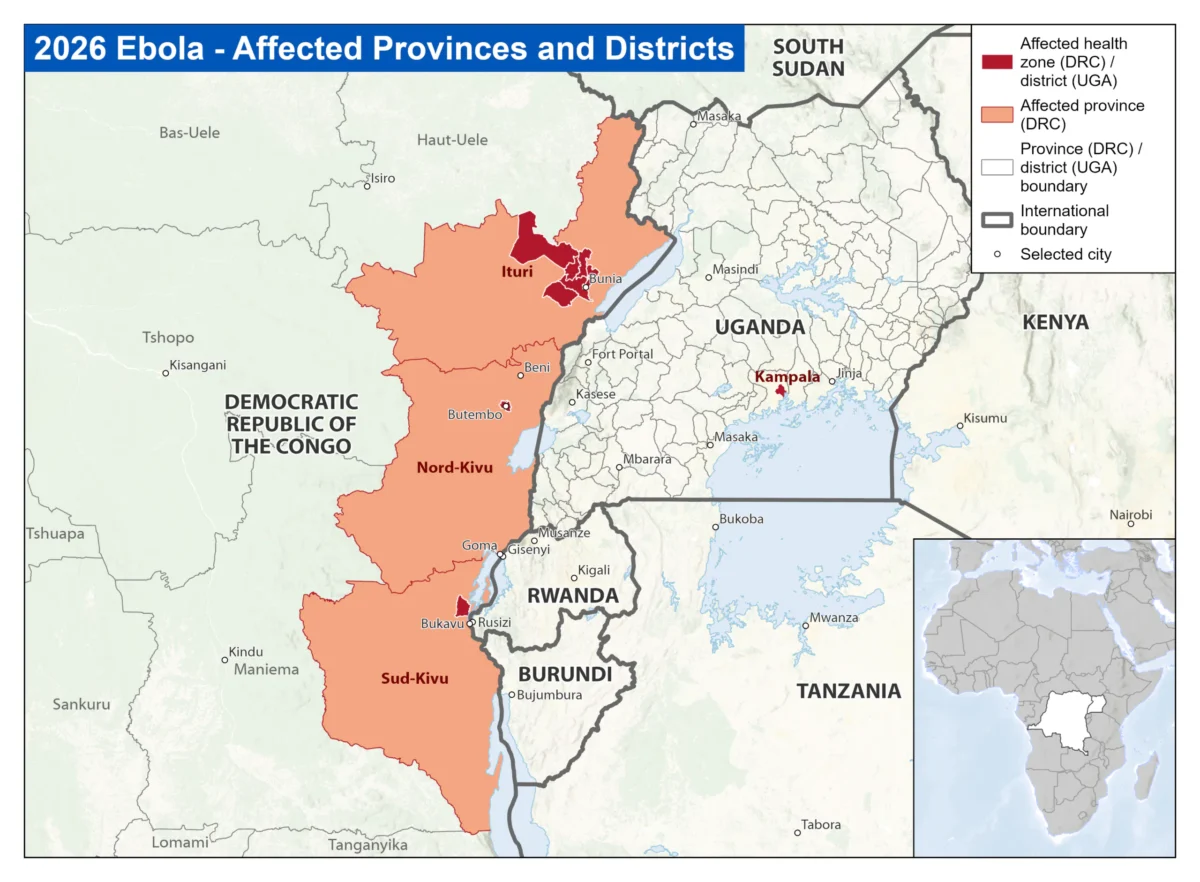
The Ebola Bundibugyo outbreak in the Democratic Republic of the Congo, as of May 23, 2026, has been confirmed in Ituri, Nord-Kivu, and Sud-Kivu provinces. Five cases related to the DRC outbreak also have been reported in Uganda's capital of Kampala. Supplied/CDC
The outbreak was first detected in the DRC’s Ituri province, where it is believed to have spread undetected for weeks. The first known case was a nurse who tested negative for the more common strain Zaire ebolavirus. She developed symptoms while working in a hospital in the capital of Bunia around April 24 and died soon after.
After that, cases were detected across the border in Uganda. While no cases have been confirmed in South Sudan, the nation is included as a precaution as the outbreak zones in eastern DRC (Ituri, North Kivu) and Uganda are just across the border.